Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
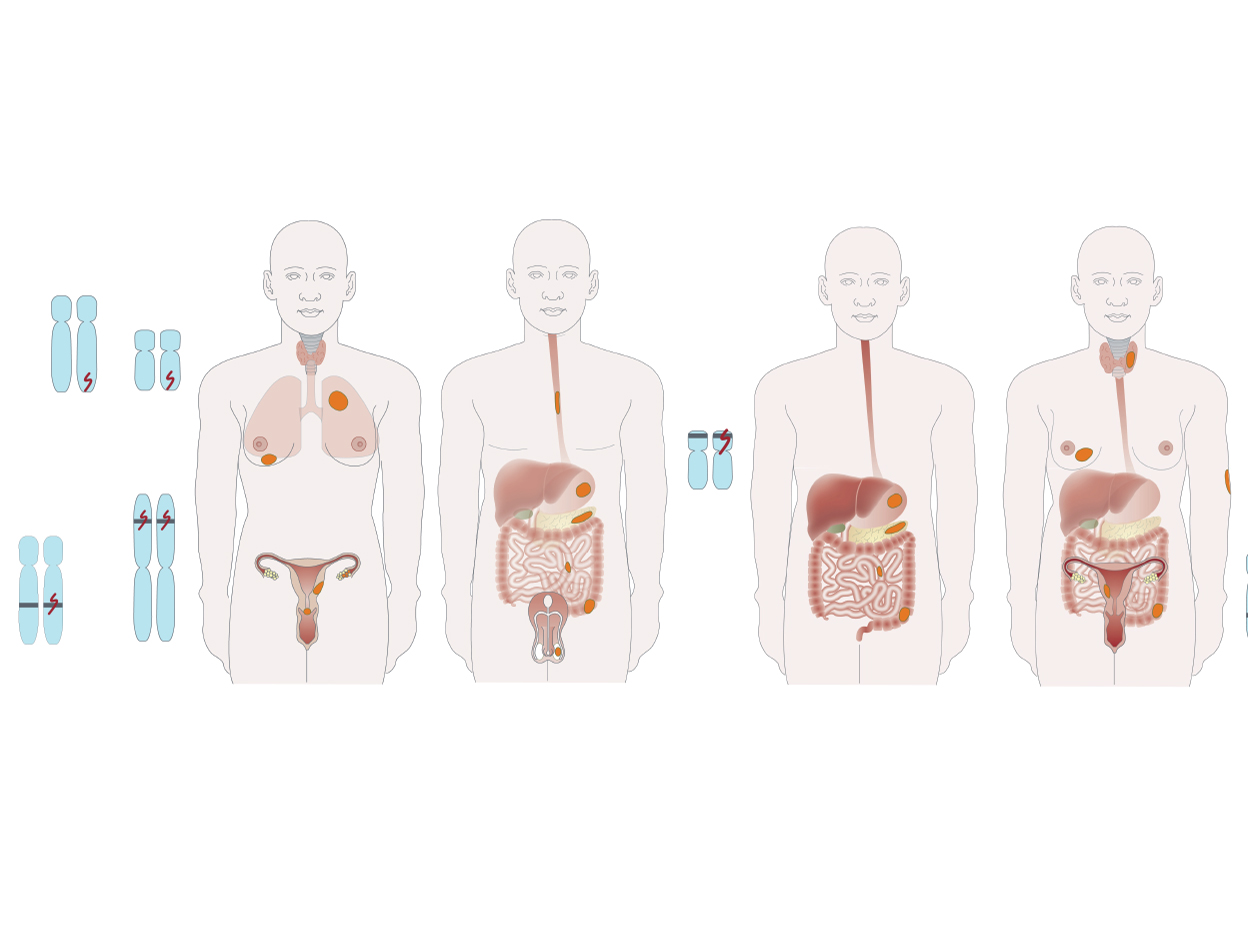
Hereditary gastrointestinal polyposis syndromes
Event
Topics
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
A primer in capsule endoscopy
Event
Topics
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Best of UEG Week - Nursing with Mary Phillips and Leigh Donnelly
Topics
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

Management of early-invasive (T1) colorectal cancer
Event
Topics
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

Endoscopic management of polyposis syndromes: European Society of Gastrointestinal Endoscopy (ESGE) guideline
Monique van leerdam, Victorine Roos, Evelien Dekker, Rodrigo Jover, Michal Filip Kaminski, Andrew Latchford, Helmut Neumann, Jean Christophe Saurin, Pieter J. Tanis, Anja Wagner, Francesc Balaguer, Luigi Ricciardiello
Publisher
Guideline
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
SURGERY AFTER ENDOSCOPIC REMOVAL OF A MALIGNANT POLYP: IS RESIDUAL DISEASE A REAL ISSUE?
Ana Isabel Ferreira 1, Joao Carlos Goncalves 1, Mariana Souto 1, Sofia Xavier 1, Pedro Boal Carvalho 1, Joana Lúcia Teixeira Magalhães Magalhães 1, José Berkeley Cotter 1
1 Hospital Senhora da Oliveira – Guimarães, Guimarães, Portugal|||School of Medicine, University of Minho, Braga, Portugal|||ICVS/3B’s, PT Government Associate Laboratory, Guimarães/Braga, Portugal
Conference
Topics
Submission format
Session
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
REACHING THE END OF THE LINE: CHARACTERIZATION OF NON-OBSTRUCTIVE DYSPHAGIA WITH NORMAL ESOPHAGEAL MOTILITY
Raquel R. Mendes 1, Jose Azevedo Rodrigues 2, André Mascarenhas 1, Helena Coelho Lima 3, Tiago Guedes 4, Silvia Maria Barrias 4, Mara Costa 5, Paulo Souto 5, João Carlos Silva 6, Joao Paulo Laranjeira Correia 6, Bárbara Morão 7, Joana Revés 7, Carina Leal 8, Rui Tato Marinho 9, Miguel Mascarenhas-Saraiva 3
1 Unidade Local de Saúde de Lisboa Ocidental, Lisbon, Portugal
2 Unidade Local de Saúde de Lisboa Ocidental, Lisbon, Portugal|||Faculdade de Medicina da Universidade de Lisboa, Lisbon, Portugal
3 ManopH, Porto, Portugal
4 Centro Hospitalar Universitário de Santo António, Porto, Portugal
5 Unidade Local de Saúde de Coimbra, Coimbra, Portugal
6 Unidade Local de Saúde Gaia e Espinho, Vila Nova de Gaia, Portugal
7 Hospital Beatriz Ângelo, Lisbon, Portugal
8 Unidade Local de Saúde de Leiria, Leiria, Portugal
9 Unidade Local de Saúde de Santa Maria, Lisbon, Portugal|||Faculdade de Medicina da Universidade de Lisboa, Lisbon, Portugal
Conference
Topics