Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Emergency upper gastrointestinal bleeding
Event
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

ROUTINE CARE DATA ANALYZED USING EXPLAINABLE ARTIFICIAL INTELLIGENCE IDENTIFY BEST THERAPEUTIC SEQUENCE OF 2ND LINE BIOLOGIC TREATMENTS AFTER A 1ST LINE WITH ANTI-TNF OR VEDOLIZUMAB IN INFLAMMATORY BOWEL DISEASE
Yoram Bouhnik 1, Pablo Iriso 2, Bastien Malahieude 3, Carmen Stefanescu 1, Chaima Romdhane 2, Yassamin BENHAYOUN SADAFYINE 1, Jawad Boulahfa 2, Laurent Peyrin-Biroulet 1, Jeremie Neuberg 3, Xavier Treton 1, Frederic Parmentier 2, Mohammad Afshar 2
1 Institut des MICI, Neuilly Sur Seine, France
2 Ariana Pharma, Paris, France
3 Instamed, Paris, France
Conference
Topics
Submission format
Session
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

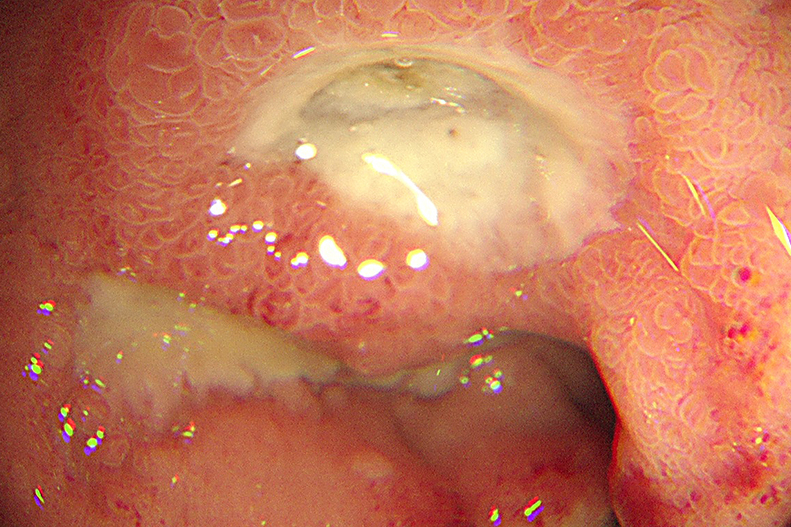
OCCURRENCE AND RISK FACTORS OF MISSED CARCINOMA IN THE UPPER GASTROINTESTINAL TRACT (PEUGIC) 2013-2023 – RETROSPECTIVE OBSERVATIONAL STUDY
1 Beskydy Gastrocentre, Frydek-Mistek, Czechia
2 Beskydy Gastrocentre, Frydek-Mistek, Czechia|||University of Ostrava, Ostrava, Czechia
3 Frydek-Mistek Hospital, Frydek-Mistek, Czechia
Conference
Topics
Submission format
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

INCIDENCE OF CHRONIC END-STAGE RENAL DISEASE IN PATIENTS WITH INFLAMMATORY BOWEL DISEASE: A POPULATION-BASED COHORT STUDY FROM THE FRENCH NATIONAL HEALTH INSURANCE DATABASE
prothe carole 1, Anastasia Boitel 1, Berenger Martin 1, Valentine Clairet 2, Lea Juif 3, Stephane Koch 3, Stephane Lang 1, Didier Ducloux 4, Maxime Desmarets 1, Lucine Vuitton 5
1 CHU Minjoz, Besançon, France
2 CHU Minjoz, Besancon, France
3 Chru Minjoz Besançon, Besancon, France
4 Chru Minjoz, Besancon, France
5 Besançon university hospital gastroenterology, Besançon, France
Conference
Topics
Submission format
Session
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

1000 PER-ORAL ENDOSCOPIC MYOTOMY AND COUNTING: AN 11-YEAR EXPERIENCE AT A SINGLE ENDOSCOPY CENTER
Rosario Landi 1, Francesca Mangiola 1, Tommaso Schepis 1, Federico Barbaro 1, Andrea Tringali 1, Vincenzo Perri 1, Guido Costamagna 1, Cristiano Spada 1, Pietro Familiari 1
1 Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Roma, Italy
Conference
Topics
Submission format
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

THE CONTRIBUTION OF THE MEDICAL EDUCATION OF THE PATIENT WITH METABOLIC-ASSOCIATED FATTY LIVER DISEASE ON THE THERAPEUTIC RESULTS
Andrei Nicolae Gologan 1, Mara-Krysta Grumeza 1, Dimitrie Stefan Gologan 1, Elena Gologan 1, Gheorghe Balan 1, Georgiana- Emmanuela Gilca-Blanariu 1
1 University of Medicine and Pharmacy Grigore T Popa, Iasi, Romania
Conference
Topics
Submission format
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

CLINICAL PERFORMANCE OF FOUR FECAL CALPROTECTIN ASSAYS FROM SMARTPHONE-BASED HOME TEST TO HIGH THROUGHPUT CENTRAL LAB METHODS
Christian Reinhard 1, Marie-Eve Ueberschlag 1, Sabine Kräuchi 1, Daniela Trapani-Vondran 1, Romain Pénager 1, Peter Kupchak 1, Laura Adina Zurbrügg 1, Thomas Schuster 1
1 BÜHLMANN Laboratories AG, Schönenbuch, Switzerland
Conference
Topics
Submission format
Session