Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
TL1a
1 Vita-Salute San Raffaele University - IRCCS San Raffaele Scientific Institute, Milan, Italy
Event
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Summary: Cancer and IBD - Mitigating risk among uncertainty
1 Charité Berlin, Berlin, Germany
Event
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
REAL-LIFE VS CLINICAL TRIAL ACCESS TO BIOLOGICAL THERAPY: FINDINGS FROM AN ITALIAN-AMERICAN STUDY ON INFLAMMATORY BOWEL DISEASE
Federica Di Vincenzo 1, Stephanie Ioannou 2, Chiara Principessa 3, Ivan Capobianco 1, Antonio Gasbarrini 4, Lucrezia Laterza 4, Maria T. Abreu 5, Franco Scaldaferri 4
1 Fondazione Policlinico Universitario "A. Gemelli" IRCCS, Università Cattolica del Sacro Cuore, Roma, Italy
2 University of Miami - Jackson Health System, Miami, United States
3 Università Cattolica del Sacro Cuore, Roma, Italy
4 Fondazione Policlinico Universitario "A. Gemelli", IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy
5 University of Miami Miller School of Medicine, Department of Medicine, Division of Gastroenterology, Miami, FL 33136; F. Widjaja Inflammatory Bowel Disease Institute, Cedars-Sinai Medical Center, Los Angeles, United States
Event
Submission format
Session
Citation
Published

Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Panel discussion: Cancer and IBD - Mitigating risk among uncertainty
Event
Topics
Citation
Published

Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Will molecular targeted therapies become the new gold-standard in PC
1 Medical University Hospital Tuebingen, Tübingen, Germany
Event
Topics
Session
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
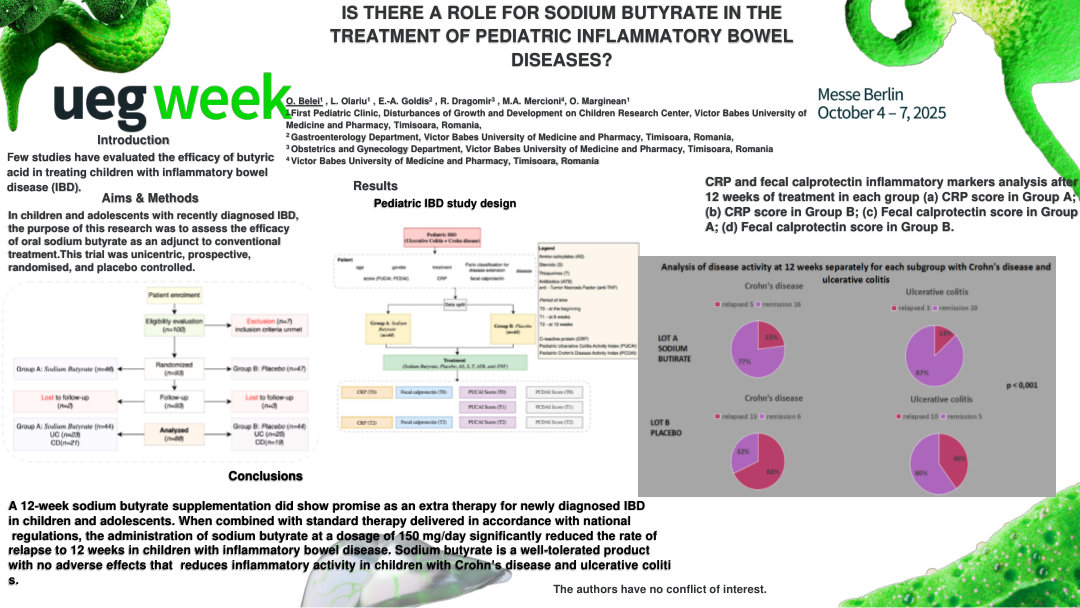
IS THERE A ROLE FOR SODIUM BUTYRATE IN THE TREATMENT OF PEDIATRIC INFLAMMATORY BOWEL DISEASES?
Oana Belei 1, Laura Olariu 1, Eugen-Adrian Goldis 1, Radu Dragomir 1, Marina Adriana Mercioni 1, Otilia Marginean 1
1 Victor Babes University of Medicine and Pharmacy, Timisoara, Romania
Conference
Topics
Submission format
Citation
Published

Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Management of pregnant women with chronic liver disease: Key points of vigilance
1 Hôpital Jean Verdier, APHP et Université Paris 13, Paris, France
Event
Topics