Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
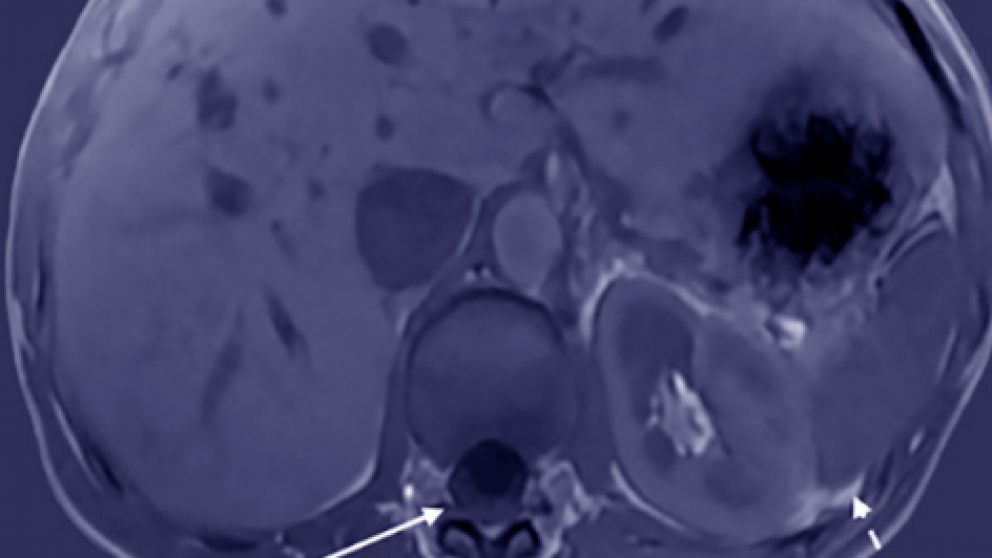
Mistakes in imaging hepatic lesions and how to avoid them
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

Endoscopic ultrasound-guided tissue sampling: European Society of Gastrointestinal Endoscopy (ESGE) Technical and Technology Review
Publisher
Guideline
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Smoking and colorectal neoplasia in patients with inflammatory bowel disease: Dose-effect relationship
1 Department of Gastroenterology, Marmara University, School Of Medicine, Istanbul, Turkey
2 UMC Utrecht, Netherlands
Topics
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
The Evolving Landscape of Scientific Publishing: Navigating Trends, Challenges, and Opportunities
1 Bradford Teaching Hospitals NHS trust, Leeds, United Kingdom
2 Amsterdam UMC, Netherlands
Topics
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
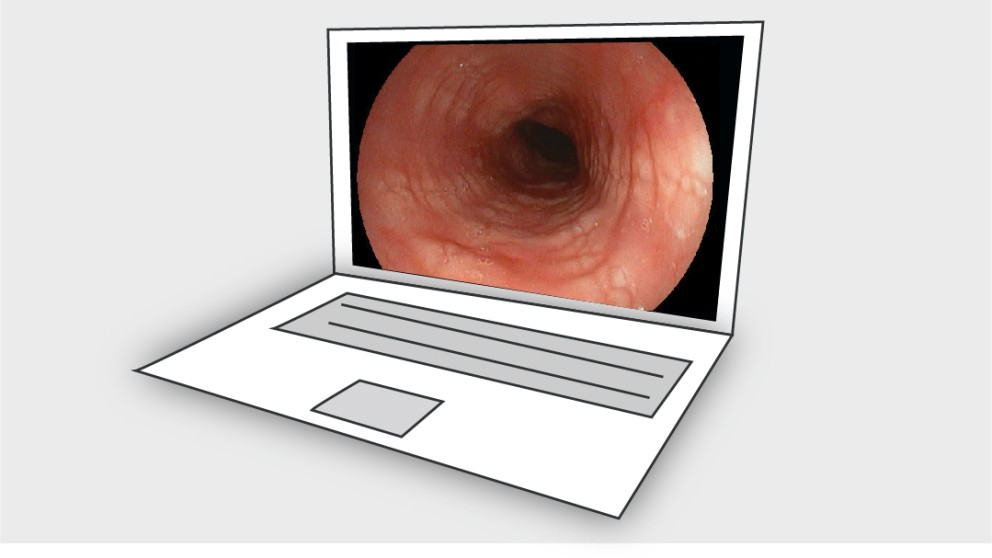
Mistakes in eosinophilic oesophagitis and how to avoid them
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Guideline for the assessment and management of gastrointestinal symptoms following colorectal surgery—A UEG/ESCP/EAES/ESPCG/ESPEN/ESNM/ESSO collaboration. Part II—Good practice guidance | sequelae to benign diseases
Publishers
Guideline
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
What are the steps for a successful clinical research career? The voyage to Ithaca
1 Department Gastroenterology, Endoscopy Unit, Hospital of the Ministry of Interior and Administration, Szczecin, Poland
2 Hospital General Universitario de Alicante, Alicante, Spain
Topics