Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
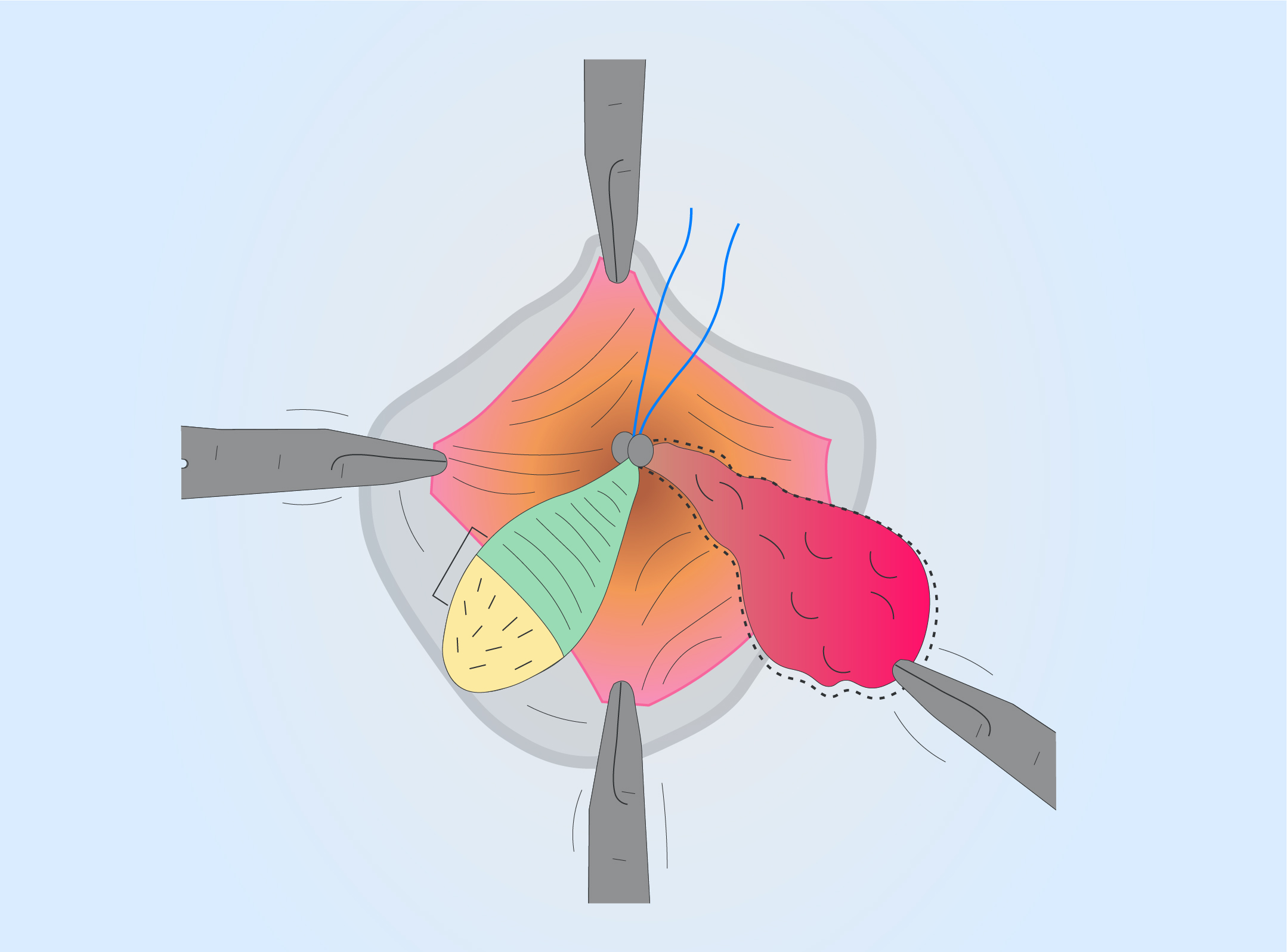
Proctology — haemorrhoids and perianal skin conditions
Event
Topics
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

Gastroenterologist's guide to stem cells
Event
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
PREDICTORS OF EOSINIPHILIC ESOPHAGITIS IN PATIENTS WITH DYSPHAGIA AND NORMAL ENDOSCOPY
Filippo Ovidi 1, Pierfrancesco Visaggi 1, Irene Solinas 1, Emanuele Marciano 2, Jason M. Dunn 3, Terence Wong 3, Edoardo Vincenzo Savarino 4, Nicola de Bortoli 1, Sebastian S. Zeki 3
1 Gastroenterology Unit, University of Pisa, Pisa, Italy
2 Azienda Ospedaliero Universitaria Pisana, Pisa, Italy
3 St Thomas' Hospital, London, United Kingdom
4 University of Padua, Division of Gastroenterology, Padua, Italy
Conference
Topics
Submission format
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
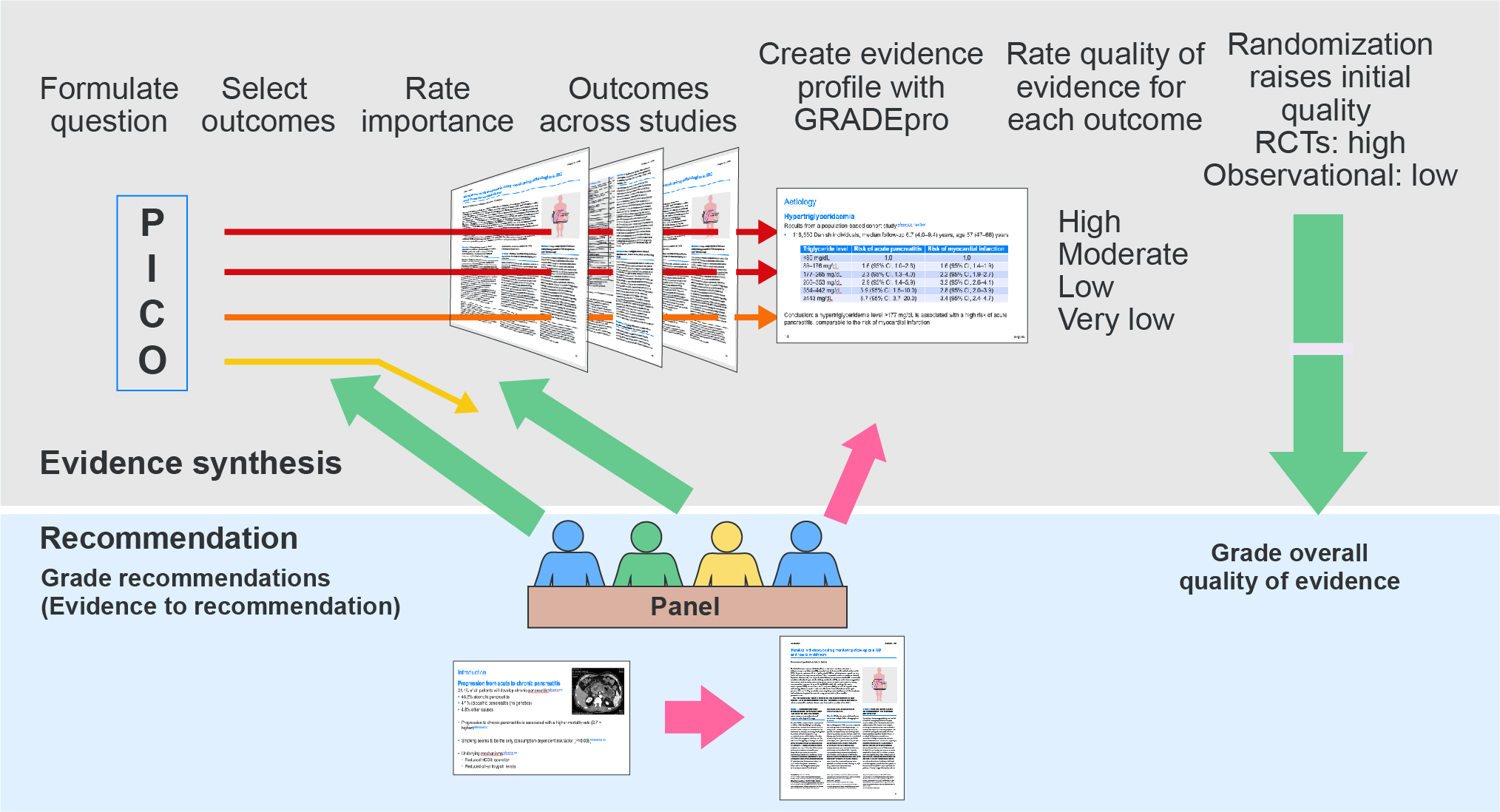
How to develop guidelines - Part 1
Event
Topics
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
EFFECT OF CELECOXIB ON SPLENOMEGALY IN CIRRHOTIC RATS BASED ON TRANSCRIPTOMIC ANALYSIS
1 Chongqing University Cancer Hospital, Chongqing, China
Conference
Topics
Submission format
Session
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
ASSOCIATIONS BETWEEN GASTROINTESTINAL SYMPTOMS, MOTILITY, AND EXTRAINTESTINAL AUTONOMIC MEASURES IN DIABETIC GASTROENTEROPATHY: A CROSS-SECTIONAL STUDY
Ditte Smed Kornum 1, Christina Brock 2, Tina Okdahl 3, Davide Bertoli 3, Huda Kufaishi 4, Anne-Marie Wegeberg 3, Katrine Lundby Høyer 1, Esben Bolvig Mark 3, Birgitte Brock 4, Christian Stevns Hansen 4, Filip K. Knop 5, Asbjørn Mohr Drewes 3, Klaus Krogh 1
1 Aarhus University Hospital, Aarhus N, Denmark
2 Aalborg Universityhospital, Aalborg, Denmark
3 Aalborg University Hospital, Aalborg, Denmark
4 Steno Diabeters Center Copenhagen, Herlev, Denmark
5 Clinical Metabolic Research at Gentofte Hospital, Copenhagen, Denmark
Conference
Topics
Submission format
Citation
Published

Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Laudatio UEG Lifetime Achievement Awardee
1 Leiden University Medical Center, Leiden, Netherlands
Event
Session