Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
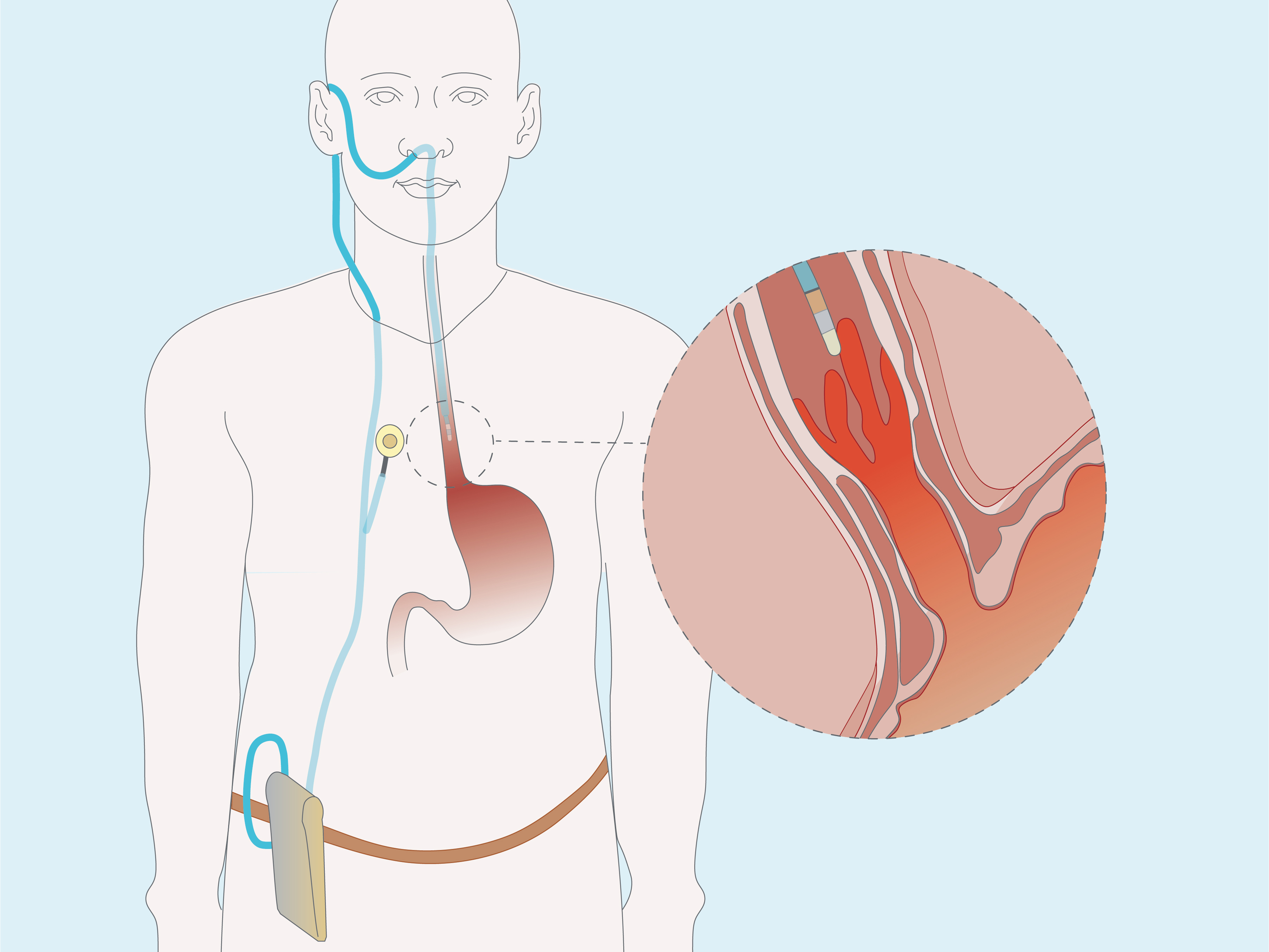
GORD Diagnosis
Event
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Towards a robust and compact deep learning system for primary detection of early Barrett’s neoplasia
1 Early Cancer Institute, University of Cambridge, United Kingdom
2 Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands
Topics
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
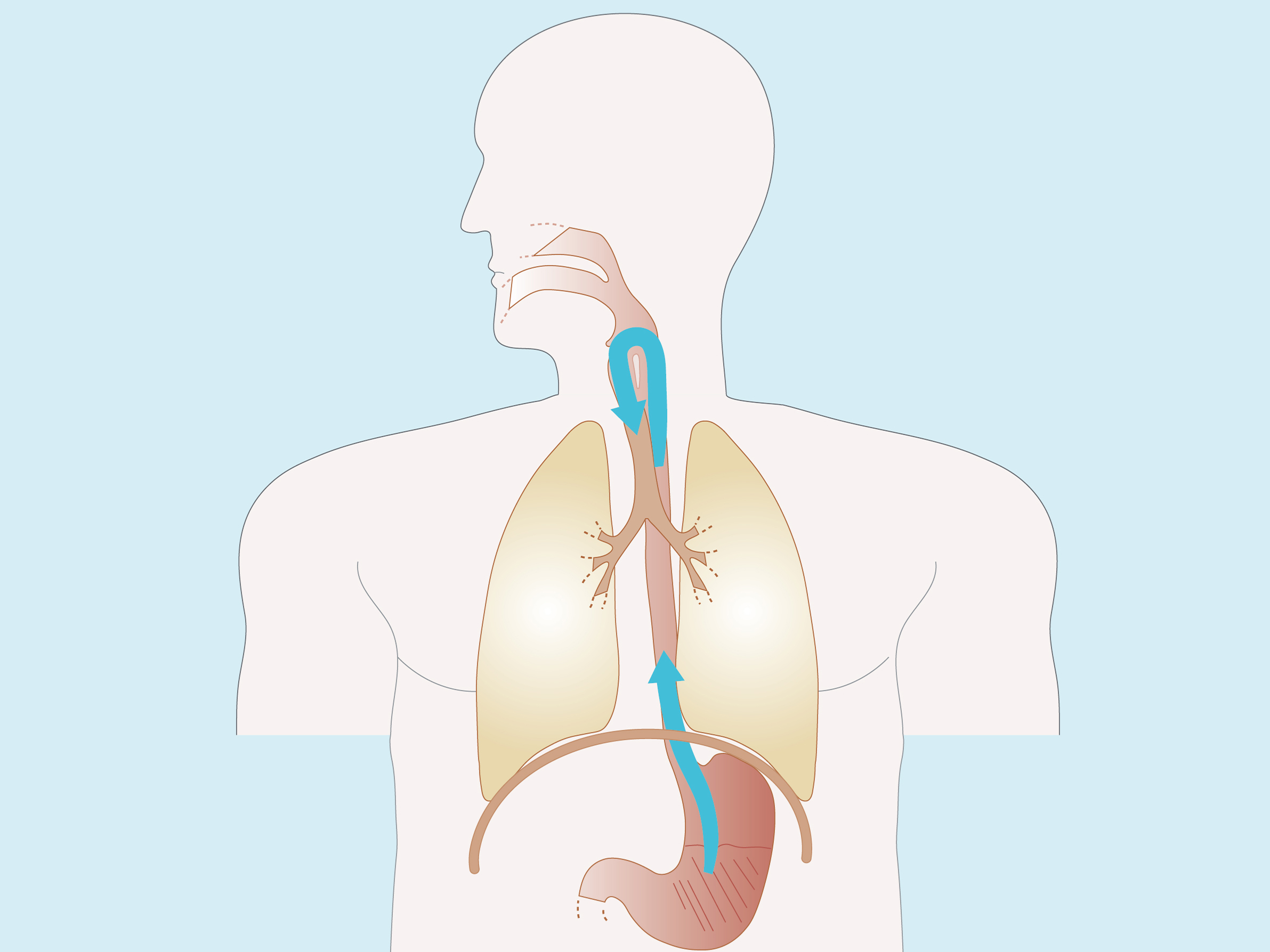
GORD Pathophysiology - Part 1
Event
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

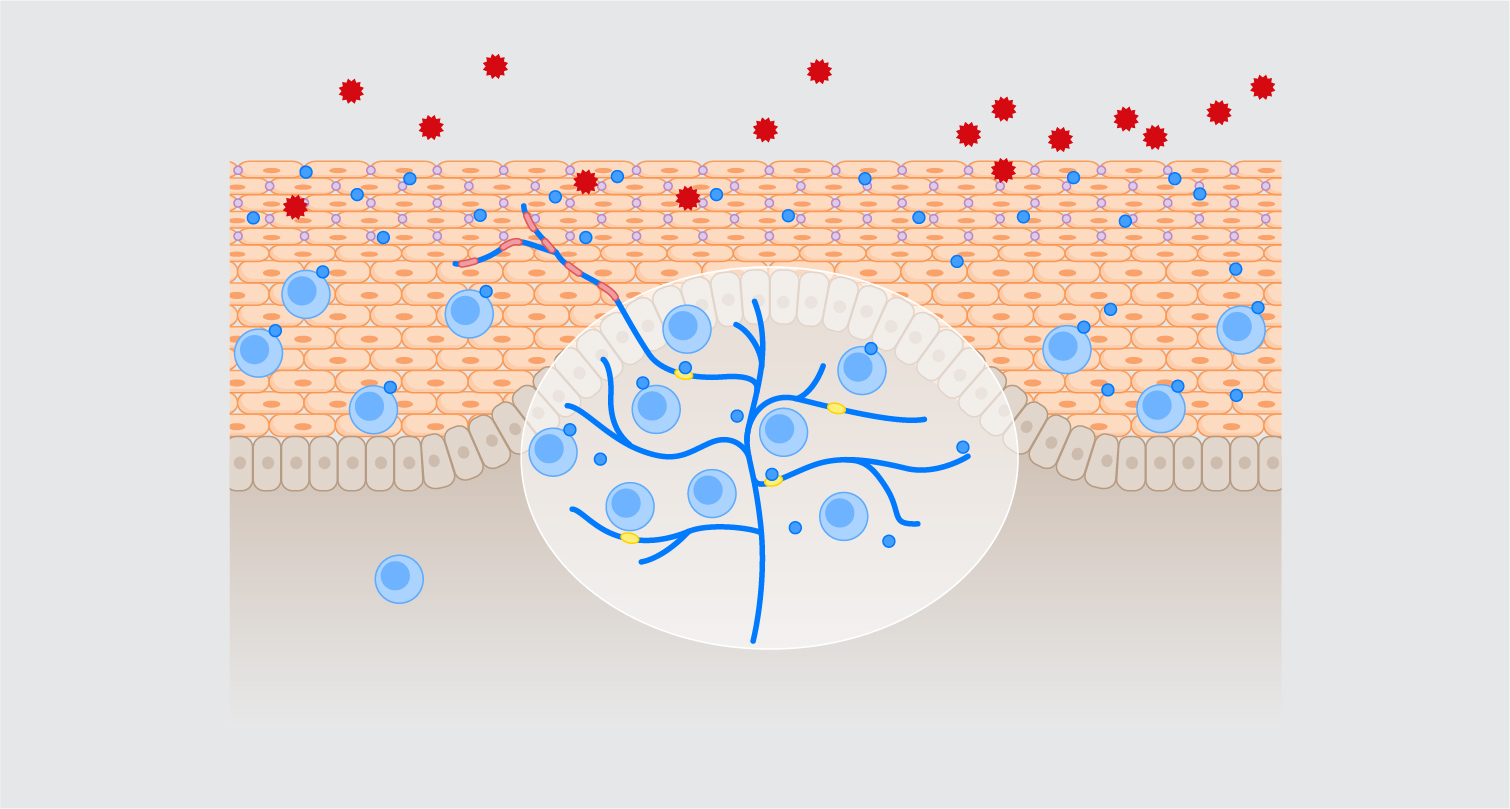
INTESTINAL EPITHELIAL AND VASCULAR PERMEABILITY IS INCREASED IN IRRITABLE BOWEL SYNDROME AND CORRELATES WITH SYMPTOMS
Maria Raffaella Barbaro 1, Cesare Cremon 2, Giovanni Marasco 1, Edoardo Vincenzo Savarino 3, Simone Guglielmetti 4, Francesca Bonomini 5, Marta Palombo 5, Antonio Di Sabatino 6, Sabrina Valente 5, Gianandrea Pasquinelli 5, Nathalie Vergnolle 7, Vincenzo Stanghellini 2, Giovanni Barbara 2
1 University of Bologna, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy
2 University of Bologna, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy
3 University of Padua, Division of Gastroenterology, Padua, Italy
4 Università degli Studi di Milano, Milano, Italy
5 University of Bologna, Bologna, Italy
6 University of Pavia, Pavia, Italy
7 INSERM UMR-1220, Toulouse, France
Conference
Topics
Submission format
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

BLUE LIGHT IMAGING IS BETTER THAN LINKED COLOR IMAGING IN THE DETECTION OF GASTRIC INTESTINAL METAPLASIA
Alice Schmal 1, Carlos Noronha Ferreira 2, Francisco Capinha 1, Francisco Faustino 1, Fabianna Rodrigues 3, Ana Teresa Carvalho 3, Heitor Siffert Pereira de Souza 4, Luís Carrilho-Ribeiro 1, Luis Correia 1
1 Centro Hospitalar Universitário Lisboa Norte/ Hospital de Santa Maria, Lisbon, Portugal
2 Centro Hospitalar Universitário Lisboa Norte/ Hospital de Santa Maria, Lisbon, Portugal|||Universidade de Lisboa/ Faculdade de Medicina de Lisboa., Lisbon, Portugal
3 Universidade Estadual do Rio de Janeiro/ Hospital Universitário Pedro Ernesto, Rio de Janeiro, Brazil
4 Universidade Federal do Rio de Janeiro/ Hospital Universitário Clementino Fraga Filho, Rio de Janeiro, Brazil
Conference
Topics
Submission format
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

LONG-TERM PROGNOSIS OF WESTERN PATIENTS AFTER ENDOSCOPIC SUBMUCOSAL DISSECTION FOR EARLY ESOPHAGEAL SQUAMOUS CELL CARCINOMA IS LIMITED DUE TO COMPETING MORTALITY
Charlotte N. Frederiks 1, Ilse Beaufort 1, Anouk Overwater 1, Lodewijk Brosens 2, Arjun D. Koch 3, Roos E. Pouw 4, Jacques J. Bergman 4, Bas L.A.M. Weusten 5
1 UMC Utrecht, Utrecht, Netherlands|||St. Antonius Hospital, Nieuwegein, Netherlands
2 UMC Utrecht, Utrecht, Netherlands
3 Erasmus Medical Center, Rotterdam, Netherlands
4 Amsterdam UMC, Amsterdam, Netherlands
5 St. Antonius Hospital, Nieuwegein, Netherlands|||UMC Utrecht, Utrecht, Netherlands
Conference
Topics
Submission format
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.