Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

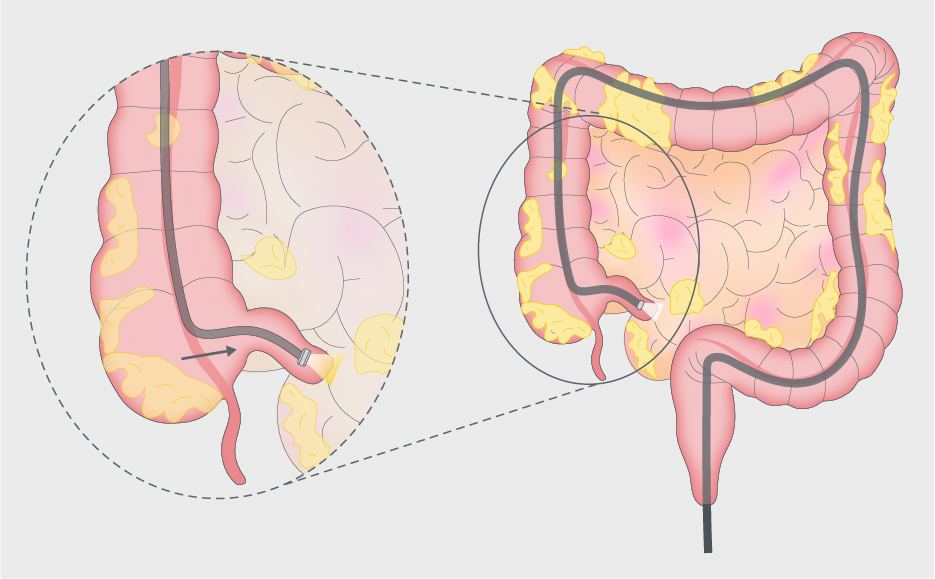
Mistakes in endoscopic resection and how to avoid them
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

Mistakes in gastrostomy insertion in children and adolescents and how to avoid them
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Mistakes in newly diagnosed Crohn's disease and how to avoid them
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
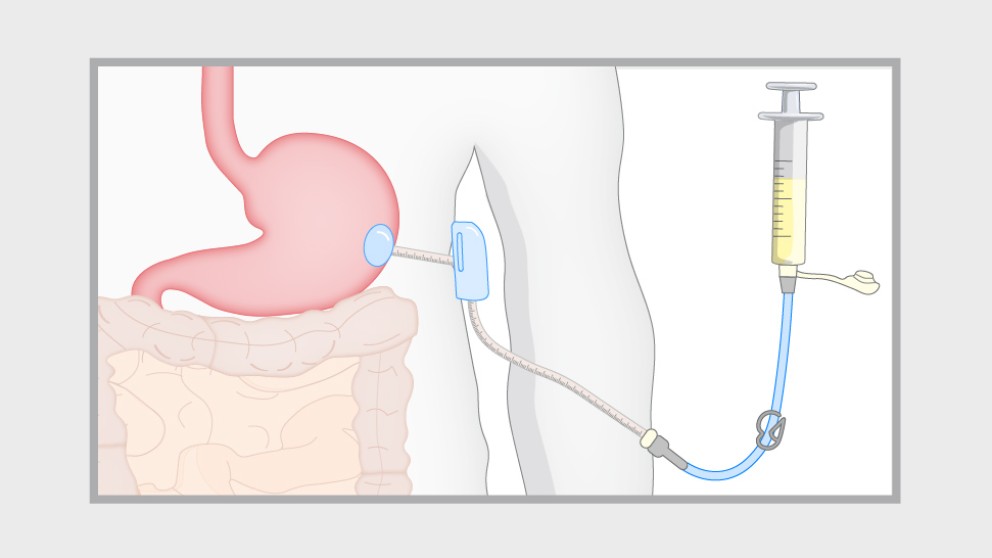
Mistakes in gastrostomy insertion and how to avoid them
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

European Society for the Study of Coeliac Disease 2025 Updated Guidelines on the Diagnosis and Management of Coeliac Disease in Adults. Part 1: Diagnostic Approach
Guideline
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Coeliac disease with David Sanders
Topics
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Transcriptomic dive into microscopic colitis
Topics