Main Recommendations
At a population level, the European Society of Gastrointestinal Endoscopy (ESGE), the European Helicobacter and Microbiota Study Group (EHMSG), and the European Society of Pathology (ESP) suggest endoscopic screening for gastric cancer (and precancerous conditions) in high-risk regions (age-standardized rate [ASR] > 20 per 100 000 person-years) every 2 to 3 years or, if cost–effectiveness has been proven, in intermediate risk regions (ASR 10–20 per 100 000 person-years) every 5 years, but not in low-risk regions (ASR < 10).
ESGE/EHMSG/ESP recommend that irrespective of country of origin, individual gastric risk assessment and stratification of precancerous conditions is recommended for first-time gastroscopy.
ESGE/EHMSG/ESP suggest that gastric cancer screening or surveillance in asymptomatic individuals over 80 should be discontinued or not started, and that patients’ comorbidities should be considered when treatment of superficial lesions is planned.
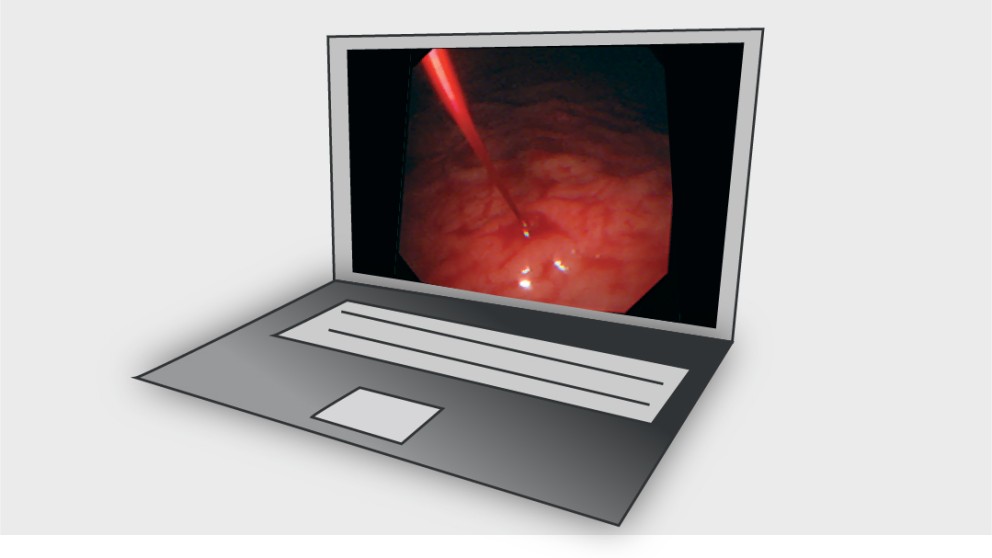
ESGE/EHMSG/ESP recommend that a high quality endoscopy including the use of virtual chromoendoscopy (VCE), after proper training, is performed for screening, diagnosis, and staging of precancerous conditions (atrophy and intestinal metaplasia) and lesions (dysplasia or cancer), as well as after endoscopic therapy. VCE should be used to guide the sampling site for biopsies in the case of suspected neoplastic lesions as well as to guide biopsies for diagnosis and staging of gastric precancerous conditions, with random biopsies to be taken in the absence of endoscopically suspected changes. When there is a suspected early gastric neoplastic lesion, it should be properly described (location, size, Paris classification, vascular and mucosal pattern), photodocumented, and two targeted biopsies taken.
ESGE/EHMSG/ESP do not recommend routine performance of endoscopic ultrasonography (EUS), computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET)-CT prior to endoscopic resection unless there are signs of deep submucosal invasion or if the lesion is not considered suitable for endoscopic resection.
ESGE/EHMSG/ESP recommend endoscopic submucosal dissection (ESD) for differentiated gastric lesions clinically staged as dysplastic (low grade and high grade) or as intramucosal carcinoma (of any size if not ulcerated or ≤ 30 mm if ulcerated), with EMR being an alternative for Paris 0-IIa lesions of size ≤ 10 mm with low likelihood of malignancy.
ESGE/EHMSG/ESP suggest that a decision about ESD can be considered for malignant lesions clinically staged as having minimal submucosal invasion if differentiated and ≤ 30 mm; or for malignant lesions clinically staged as intramucosal, undifferentiated and ≤ 20 mm; and in both cases with no ulcerative findings.
ESGE/EHMSG/ESP recommends patient management based on the following histological risk after endoscopic resection:
Curative/very low-risk resection (lymph node metastasis [LNM] risk < 0.5 %–1 %): en bloc R0 resection; dysplastic/pT1a, differentiated lesion, no lymphovascular invasion, independent of size if no ulceration and ≤ 30 mm if ulcerated. No further staging procedure or treatment is recommended.
Curative/low-risk resection (LNM risk < 3 %): en bloc R0 resection; lesion with no lymphovascular invasion and: a) pT1b, invasion ≤ 500 µm, differentiated, size ≤ 30 mm; or b) pT1a, undifferentiated, size ≤ 20 mm and no ulceration. Staging should be completed, and further treatment is generally not necessary, but a multidisciplinary discussion is required.
Local-risk resection (very low risk of LNM but increased risk of local persistence/recurrence): Piecemeal resection or tumor-positive horizontal margin of a lesion otherwise meeting curative/very low-risk criteria (or meeting low-risk criteria provided that there is no submucosal invasive tumor at the resection margin in the case of piecemeal resection or tumor-positive horizontal margin for pT1b lesions [invasion ≤ 500 µm; well-differentiated; size ≤ 30 mm, and VM0]). Endoscopic surveillance/re-treatment is recommended rather than other additional treatment.
High-risk resection (noncurative): Any lesion with any of the following: (a) a positive vertical margin (if carcinoma) or lymphovascular invasion or deep submucosal invasion (> 500 µm from the muscularis mucosae); (b) poorly differentiated lesions if ulceration or size > 20 mm; (c) pT1b differentiated lesions with submucosal invasion ≤ 500 µm with size > 30 mm; or (d) intramucosal ulcerative lesion with size > 30 mm. Complete staging and strong consideration for additional treatments (surgery) in multidisciplinary discussion.
ESGE/EHMSG/ESP suggest the use of validated endoscopic classifications of atrophy (e. g. Kimura–Takemoto) or intestinal metaplasia (e. g. endoscopic grading of gastric intestinal metaplasia [EGGIM]) to endoscopically stage precancerous conditions and stratify the risk for gastric cancer.
ESGE/EHMSG/ESP recommend that biopsies should be taken from at least two topographic sites (2 biopsies from the antrum/incisura and 2 from the corpus, guided by VCE) in two separate, clearly labeled vials. Additional biopsy from the incisura is optional.
ESGE/EHMSG/ESP recommend that patients with extensive endoscopic changes (Kimura C3 + or EGGIM 5 +) or advanced histological stages of atrophic gastritis (severe atrophic changes or intestinal metaplasia, or changes in both antrum and corpus, operative link on gastritis assessment/operative link on gastric intestinal metaplasia [OLGA/OLGIM] III/IV) should be followed up with high quality endoscopy every 3 years, irrespective of the individual’s country of origin.
ESGE/EHMSG/ESP recommend that no surveillance is proposed for patients with mild to moderate atrophy or intestinal metaplasia restricted to the antrum, in the absence of endoscopic signs of extensive lesions or other risk factors (family history, incomplete intestinal metaplasia, persistent H. pylori infection). This group constitutes most individuals found in clinical practice.
ESGE/EHMSG/ESP recommend H. pylori eradication for patients with precancerous conditions and after endoscopic or surgical therapy.
ESGE/EHMSG/ESP recommend that patients should be advised to stop smoking and low-dose daily aspirin use may be considered for the prevention of gastric cancer in selected individuals with high risk for cardiovascular events.