Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Gastrointestinal Neuroendocrine Tumours
Event
Topics
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

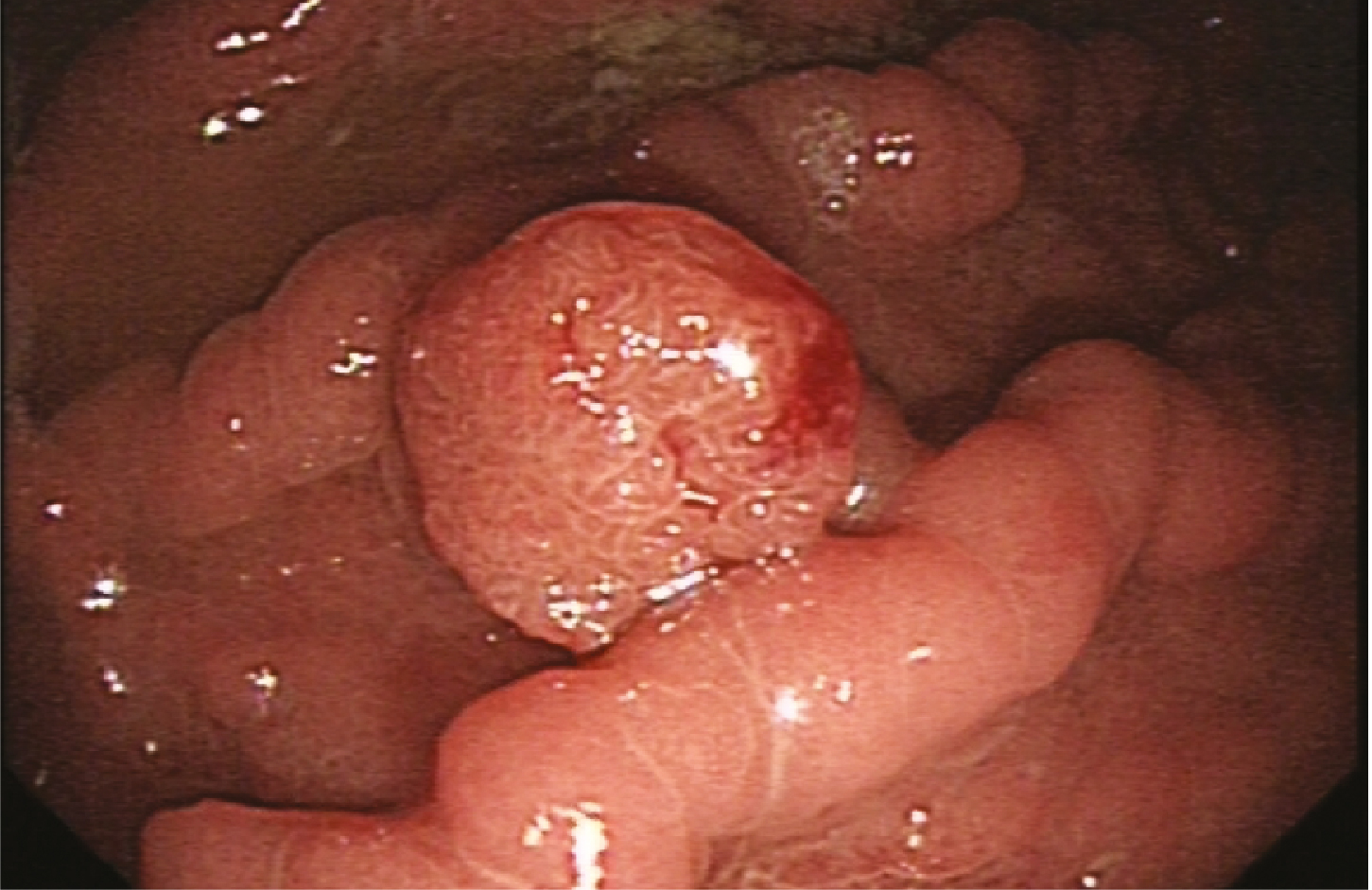
Management of early-invasive (T1) colorectal cancer
Event
Topics
Accreditation status
Duration
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Best of UEG Week - Nursing with Mary Phillips and Leigh Donnelly
Topics
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.

European Society for the Study of Coeliac Disease (ESsCD) 2025 Updated Guidelines on the Diagnosis and Management of Coeliac Disease in Adults. Part 2: Management, Follow-Up, and Complex Disease Courses
Guideline
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
REAL-LIFE VS TRIAL ACCESS TO BIOLOGICAL THERAPY DIFFERENCES: A 2019-2020 EXPERIENCE IN AN ITALIAN TERTIARY IBD CENTER
Federica Di Vincenzo 1, Rossella Maresca 1, Vincenzina Mora 1, Valentina Petito 1, Pierluigi Puca 1, Maria Caterina Russo 1, Laura Turchini 1, Valeria Amatucci 1, Daniele Napolitano 1, Elisa Schiavoni 1, Laura Parisio 1, Carlo Romano Settanni 1, Marco Pizzoferrato 2, Loris Riccardo Lopetuso 1, Alessandro Armuzzi 3, Daniela Pugliese 1, Antonio Gasbarrini 4, Lucrezia Laterza 1, Franco Scaldaferri 4
1 Fondazione Policlinico Universitario “A. Gemelli” IRCCS, Roma, Italy
2 UOC Medicina Gastroenterologia, Roma, Italy
3 IBD Center, IRCCS Humanitas Research Hospital, Rozzano, Milan, Italy
4 Catholic University of Rome Dept. of Internal Medicine Dept. of Gastroenterology, Roma, Italy
Conference
Topics
Submission format
Session
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
BETWEEN VISION AND REALITY: RESULTS FROM A PAN-EUROPEAN SURVEY ON ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY TRAINING CONDITIONS
Karim Hamesch 1, Oscar Cahyadi 2, Stavros Dimitriadis 3, Marcus Hollenbach 4, Pilar Acedo 5, Myriam Ayari 6, Helena Tammela 7, Egle Dieninyte - Misiune 8, Viktor Domislovic 9, Ana Dugic 10, Martin Ďuriček 11, Omar Elshaarawy 12, Anne Fennessy 13, Mark Enrik Geissler 14, Zornitsa Gorcheva 15, Amer Hadi 16, Valon Hamza 17, Ismar Hasukic 18, Henriette Heinrich 19, Iris J. M. Levink 20, Jan Král 21, Lumir Kunovsky 22, Mattias Mandorfer 23, Maria Moris 24, Yana Nikiforova 25, Hassan ouaya 26, Gianluca Pellino 27, Anthea Pisani 28, Odri Qejvani 29, Hasan Sadigov 30, Maciej Salaga 31, Orestis Sidiropoulos 32, Cem Simsek 33, Paula Sousa 34, Milica Stojkovic Lalosevic 35, Katja Tepeš 36, Andrei Mihai Voiosu 37, Lucas Wauters 38, Alberto Zanetto 39, Sophie Schlosser-Hupf 40, Jonas J. Staudacher 41
1 University Hospital Aachen, Aachen, Germany|||University Hospital RWTH Aachen, Aachen, Germany|||Junge Gastroenterologie (JuGa) - German Young Gastroenterology Study Group, Berlin, Germany
2 St. Josef-Hospital, a hospital of the Ruhr-University-Bochum, Essen, Germany|||Junge Gastroenterologie (JuGa) - German Young Gastroenterology Study Group, Berlin, Germany
3 University Hospital Coventry and Warwickshire, Coventry, United Kingdom|||Junge Gastroenterologie (JuGa) - German Young Gastroenterology Study Group, Berlin, Germany
4 Heidelberg University Hospital, Heidelberg, Germany|||Junge Gastroenterologie (JuGa) - German Young Gastroenterology Study Group, Berlin, Germany
5 University College London, London, United Kingdom
6 Internal Security Forces Hospital La Marsa, Tunis, Tunisia
7 East Tallinn Central Hospital, Tallinn, Estonia
8 Vilnius university Santaros Klinikos, Vilnius, Lithuania|||Vilnius university hospital Santara Clinics, Vilnius, Lithuania
9 University Hospital Centre Zagreb, Zagreb, Croatia
10 Heidelberg University Hospital, Department of Medicine IV, Heidelberg, Germany, Heidelberg, Germany|||Karolinska Institute, Stockholm, Sweden|||Junge Gastroenterologie (JuGa) - German Young Gastroenterology Study Group, Berlin, Germany
11 Jessenius Faculty of Medicine, University Hospital in Martin, Martin, Slovakia
12 Royal Liverpool University Hospital, UK, Liverpool, United Kingdom|||National Liver Institute, Menoufia University, Menoufia, Egypt
13 St Vincent's University Hospital, Dublin 14, Ireland
14 Medical Faculty and University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany|||Junge Gastroenterologie (JuGa) - German Young Gastroenterology Study Group, Berlin, Germany
15 Saint Marina University Hospital, Pleven, Bulgaria
16 Hvidovre University Hospital, Soeborg, Denmark
17 University Clinical Center of Kosova, Prishtine, Kosovo
18 UKC Tuzla, Tuzla, Bosnia and Herzegovina
19 Universitätsspital Basel, Basel, Switzerland
20 Erasmus University Medical Center, Rotterdam, Netherlands
21 Institute for Clinical and Experimental Medicine, Prague, Czechia|||Second Faculty of Medicine, Charles University, Prague, Czechia
22 2nd Department of Internal Medicine – Gastroenterology and Geriatrics, University Hospital Olomouc, Faculty of Medicine, Palacky University Olomouc, Olomouc, Czechia|||University Hospital Olomouc, Faculty of Medicine and Dentistry, Olomouc, Czechia|||Masa
23 Medical University of Vienna, Vienna, Austria
24 Hospital Universitario Marqués de Valdecilla, Santander, Spain
25 Government Institution “L.T.Malaya Therapy National Institute of the National Academy of Medical Sciences of Ukraine”, Kharkov, Ukraine
26 tangier faculty of medicine / tangier mohamed VI university hospital, Tangier, Morocco
27 Università degli Studi della Campania "Luigi Vanvitelli", Aversa (CE), Italy|||Vall d'Hebron University Hospital, Universitat Autonoma de Barcelona UAB, Barcelona, Spain
28 Mater Dei Hospital, Mosta, Malta
29 University Hospital Center 'Mother Teresa', Tirana, Albania
30 AZERBAIJAN MEDICAL UNIVERSITY, Baku, Azerbaijan
31 Medical University of Lodz, Lodz, Poland
32 417 NIMTS, Cholargos, Greece
33 Hacettepe University, Ankara, Turkey
34 Tondela-Viseu Hospital Center, Viseu, Portugal
35 Clinical center of Serbia, Belgrade, Serbia
36 Diagnostic center Rogaska, Rogaska Slatina, Slovenia
37 Colentina Clinical Hospital Dept. of Gastroenterology, Bucharest, Romania
38 University Hospitals Leuven, Leuven, Belgium
39 Gastroenterology/Multivisceral Transplant Unit, Padua, Italy
40 Universitätsklinikum Regensburg, Regensburg, Germany|||Junge Gastroenterologie (JuGa) - German Young Gastroenterology Study Group, Berlin, Germany
41 Charité Universitätsmedizin Berlin, Berlin, Germany|||Berlin Institute of Health at Charité, Berlin, Germany
Conference
Topics
Submission format
Session
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
A SIMPLIFIED APPROACH TO PERCUTANEOUS ENDOSCOPIC GASTROSTOMY (PEG) TUBE PLACEMENT IN AMYOTROPHIC LATERAL SCLEROSIS (ALS) PATIENTS – SAFETY AND COMPLICATIONS
1 Tel-Aviv Sourasky Medical center, Tel-aviv, Israel|||Tel-Aviv University, Tel-Aviv, Israel
Conference
Topics
Submission format
Session