Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
MULTICENTER, RANDOMIZED NON-INFERIORITY TRIAL COMPARING TRANSANAL MINIMAL INVASIVE SURGERY (TAMIS) AND ENDOSCOPIC SUBMUCOSAL DISSECTION (ESD) FOR RESECTION OF NON-PEDUNCULATED RECTAL LESIONS (TRIASSIC STUDY)
Nik Dekkers 1, Daan Verhoeven 1, Jurjen J. Boonstra 1, Leon M.G. Moons 2, Roel Hompes 3, Barbara A.J. Bastiaansen 3, Jurriaan B. Tuynman 3, Arjun D. Koch 4, Bas L.A.M. Weusten 5, Alaa Alkhalaf 6, Eric J. T. Belt 7, Wilhelmus A. Bemelman 3, Esther C.J. Consten 8, Stijn Crobach 1, Richard Dang 1, Paul Didden 2, Brechtje Grotenhuis 9, Hakimullah Hekmat 10, Elmer Hoekstra 11, Wilbert B. van den Hout 1, Inge Huibregtse 9, Josbert J. Keller 12, jolein van der Kraan 1, Alexandra Langers 1, Monique van leerdam 13, Andreas W.K.S. Marinelli 12, Peter A. Neijenhuis 14, Jikke M.T. Omloo 15, Apollo Pronk 16, Robert Roomer 17, Mar Rodríguez–Girondo 1, Ruud W. M. Schrauwen 18, Matthijs P. Schwartz 8, Mareille Verseveld 17, Wouter De Vos Tot Nederveen Cappel 6, Bob J. van Wely 18, Marinke Westerterp 12, Erik Van Westreenen 6, Eelco J.R. de Graaf 10, Jonathan Y.L. Lai 12, Rogier Ten Hove 14, Hans F.A. Vasen 1, Pascal G. Doornebosch 10, James Hardwick 1
1 Leiden University Medical Center, Leiden, Netherlands
2 University Medical Center Utrecht, Utrecht, Netherlands
3 Amsterdam UMC, Amsterdam, Netherlands
4 Erasmus MC Cancer Institute, Rotterdam, Netherlands
5 St Antonius Hospital, Nieuwegein, Netherlands
6 Isala Clinics, Zwolle, Netherlands
7 Albert Schweitzer Hospital, Dordrecht, Netherlands
8 Meander Medical Center, Amersfoort, Netherlands
9 Netherlands Cancer Institute, Amsterdam, Netherlands
10 IJsselland Hospital, Capelle aan den IJssel, Netherlands
11 Hagaziekenhuis, The Hague, Netherlands
12 Haaglanden Medical Center, The Hague, Netherlands
13 Netherlands Cancer Institute, Amsterdam, Netherlands|||Leiden University Medical Center, Leiden, Netherlands
14 Alrijne Hospital, Leiderdorp, Netherlands
15 Gelre Hospitals, Apeldoorn, Netherlands
16 Diakonessenhuis, Utrecht, Netherlands
17 Franciscus Gasthuis, Rotterdam, Netherlands
18 Bernhoven Hospital, Uden, Netherlands
Event
Topics
Submission format
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
UEG Journal Best Paper Award
1 Uni Marburg, Marburg, Germany
Event
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
AIP 1 and IgG-4 related disorders
1 San Raffaele University, San Raffaele, Italy
Event
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
GP: When to refer?
1 Ospedale Sandro Pertini, Roma, Roma, Italy
Event
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Undertstanding genetic causes of liver and bile duct diseases: Treatment implications
1 University Hospital Magdeburg, Magdeburg, Germany
Event
Session
Citation
Published

Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Oligometastasitc disease: Does surgical resection play a role?
1 Universitätsklinikum Köln, Köln, Germany
Event
Topics
Session
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
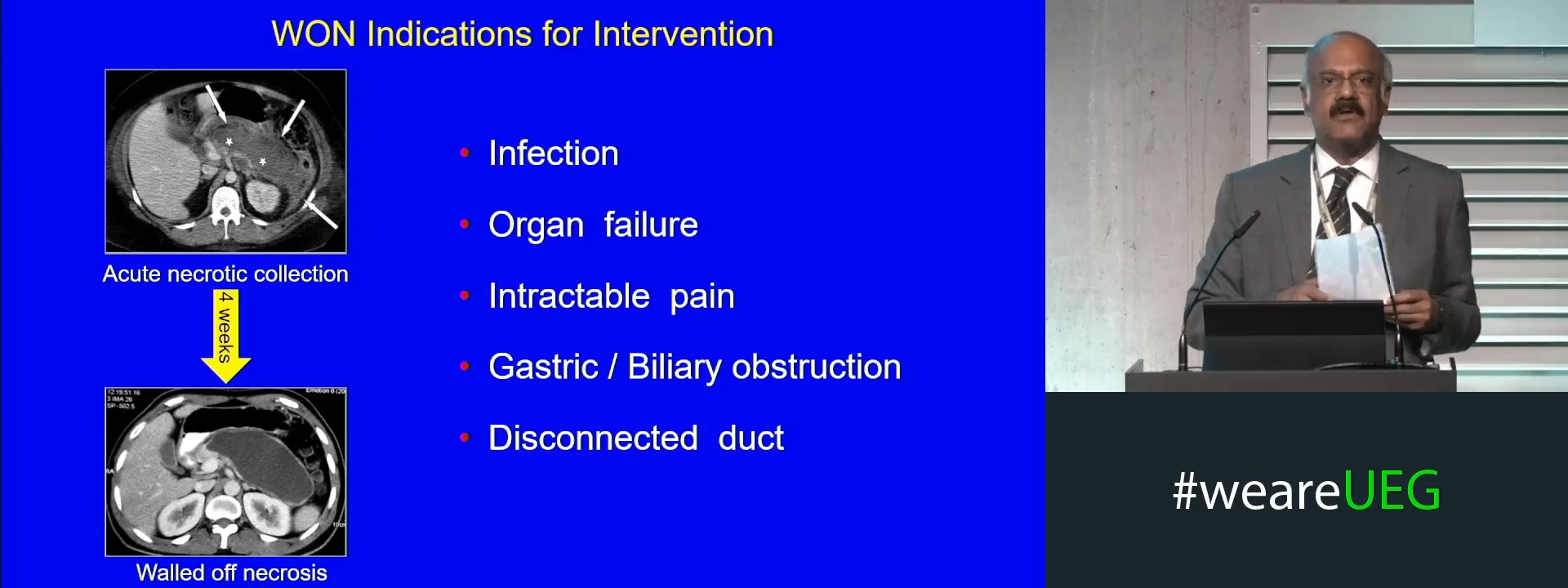
Early versus delayed endoscopic necrosectomy (Complete Session)
Event
Topics