Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
BILE LIQUID BIOPSY IN PANCREATOBILIARY TUMORS: A NOVEL APPROACH TO DETECT ACTIONABLE MUTATIONS
Javier Rández-Garbayo 1, Maria Rullan Iriarte 2, Diary Fall 3, Silvia Pinto Martínez 2, Patricia de Miguel 2, David Ruiz-Clavijo Garcia 2, Belen GONZÁLEZ DE LA HIGUERA CARNICER 2, Federico Bolado Concejo 2, Daniel Oyón 4, Irene Amat 2, David Guerrero-Setas 2, Ana Purroy 1, Juan Carrascosa Gil 2, Vanesa Jusué Irurita 2, Ignacio Fernández-Urién Sainz 2, María Arechederra 5, Carmen Berasain 5, Juan Jose Vila 2, Matias A. Avila 5, Jesús M. Urman 2
1 Navarrabiomed, Pamplona, Spain|||Navarra Institute for Health Research, IdiSNA, Pamplona, Spain
2 Navarra University Hospital, Pamplona, Spain|||Navarra Institute for Health Research, IdiSNA, Pamplona, Spain
3 Navarra University Hospital, Pamplona, Spain
4 Hospital General Universitario Gregorio Marañón, Madrid, Spain|||Navarra Institute for Health Research, IdiSNA, Pamplona, Spain
5 Center of Applied Medicine (CIMA) / University of Navarra, Pamplona, Spain|||Navarra Institute for Health Research, IdiSNA, Pamplona, Spain
Event
Submission format
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
HCC: Novel treatment options in advanced diseases
1 LMU Munich, Munich, Germany
Event
Citation
Published

Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
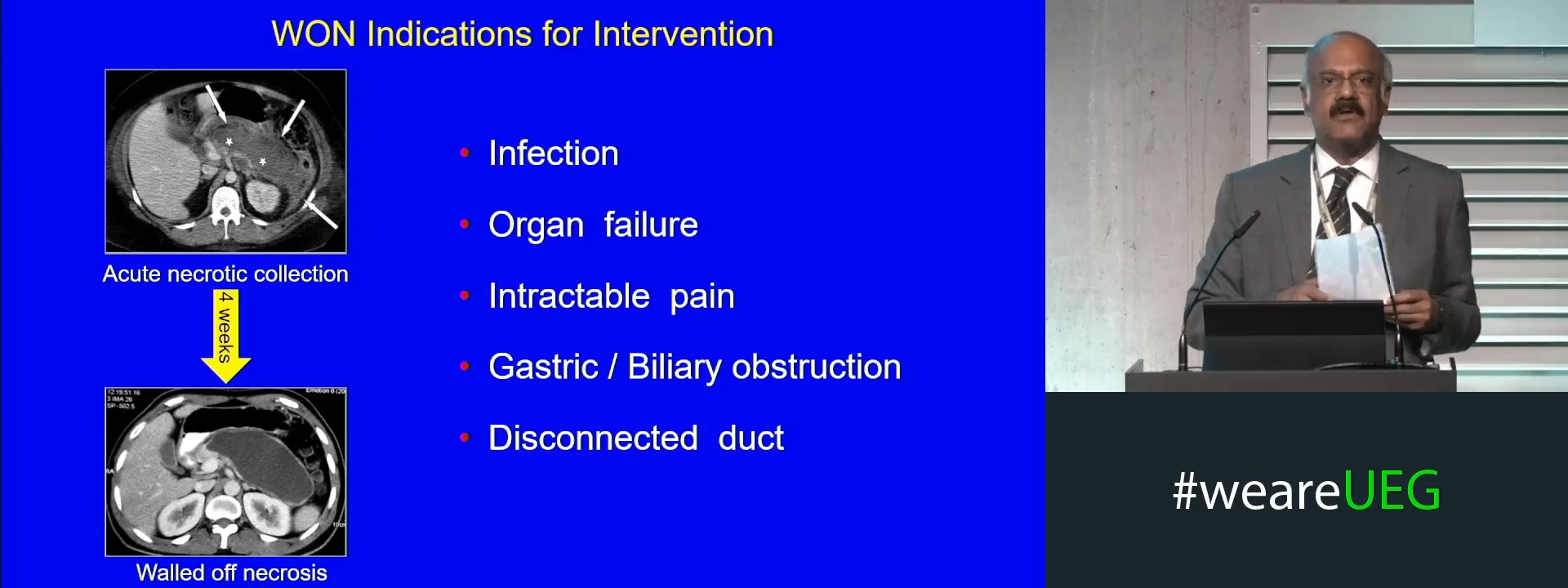
Pancreas necrosis: What to do after initial drainage
1 St. Antonius Ziekenhuis, Nieuwegein, Netherlands
Event
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Early versus delayed endoscopic necrosectomy (Complete Session)
Event
Topics
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Difficult stones: Is it the stone or the endoscopist?
1 San Matteo Hospital, Pavia, Italy
Event
Topics
Citation
Published

Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Acute pancreatitis: When to reserve an ITU bed?
1 University Hospital LMU Munich, München, Germany
Event
Topics
Session
Citation
Published
Log in to access this content.
Free for all myUEG account holders. Your access level is set automatically based on your occupation. Medical professionals get full access to all content. If you are a non-medical user, you can only access UEG Week content from congresses you attended.
Not sure what you can access? Learn more about account types.
Does autoimmune pancreatitis type III exist?
1 Institute of Molecular Oncology and Stem Cell Biology, Ulm University Hospital, Ulm, Germany
Event
Topics